


Introduction: Tyrosine kinase inhibitor therapy has been associated with cardiovascular (CV) events. BOS is approved for patients (pts) with newly diagnosed Philadelphia chromosome-positive (Ph+) chronic phase (CP) CML and Ph+ CML resistant/intolerant to prior therapy. We analyzed cardiac, vascular and hypertension treatment-emergent adverse events (TEAEs) in pts with newly diagnosed CP CML receiving BOS or IMA after 5 yrs follow-up in BFORE.
Methods: In the open-label, phase 3 BFORE trial (NCT02130557), 536 pts with newly diagnosed CP CML were randomized 1:1 to receive first-line 400 mg once-daily BOS (n=268) or IMA (n=268; 3 untreated). The current analysis included all pts who received ≥1 dose of study drug. TEAEs were monitored from first dose of study drug until 28 d after last dose; monitoring of non-serious adverse events (AE) ended at the start of a new cancer treatment. Prespecified MedDRA terms (cardiac, n=133; vascular, n=502) comprised clusters of investigator-assessed TEAEs (Table). Multivariable proportional subdistribution hazard models predicting time to first TEAE included treatment group; baseline demographic information; history of cardiac events, vascular events, hypertension, diabetes, hyperlipidemia, and tobacco use; as well as hypertension, cardiac (for vascular model) and vascular (for cardiac model) TEAEs. CI excluding 1 was considered predictive of outcome. This analysis was based on 17-Apr-20 last pt last visit (12-Jun-20 database lock), 5 y (240 wks) after last enrolled pt.
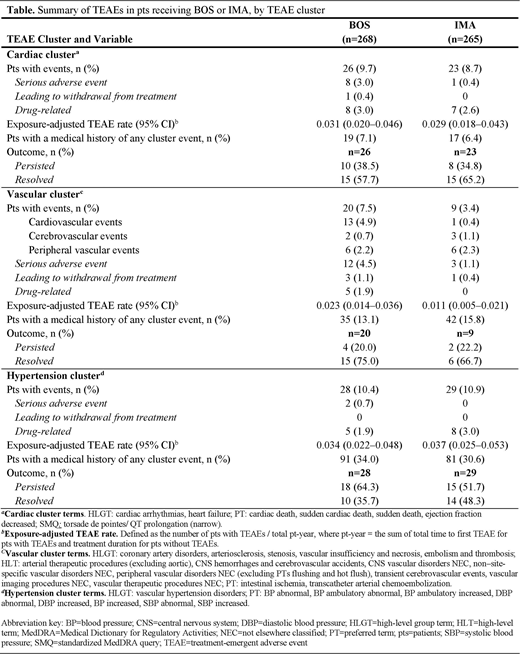
Results: At study completion, 59.7% of BOS pts and 58.1% of IMA pts were still on treatment. Median duration of treatment was 55 mo for pts receiving BOS or IMA; respective median (range) dose intensity was 393.6 (39-583) vs 400.0 (189-765) mg/d. In the BOS vs IMA arm, 57.8% vs 56.2% of pts had ≥1 CV risk factor at baseline; 20.9% vs 17.7% had ≥3 risk factors, respectively. The most common risk factors were a history of hypertension (BOS, 34.0%; IMA, 30.6%), BMI >30 (BOS, 23.1%; IMA, 21.9%), age ≥65 y (BOS, 19.8%; IMA, 17.4%), and history of hyperlipidemia (BOS, 16.8%; IMA, 18.9%). Rates of cardiac, vascular and hypertension TEAEs; serious adverse events (AEs); AEs leading to treatment withdrawal and drug-related TEAEs (per investigator) were low in both arms (Table). Exposure-adjusted rates of cardiac, vascular and hypertension TEAEs were similar between arms (Table). Risk factors for cardiac TEAEs (HR; 95% CI) were age in years (1.04 [1.02-1.07]), race other than Asian or black compared to white (<0.01 [<0.01-<0.01]), a history of tobacco use (6.94 [1.89-25.40]) and cardiac events (3.59 [1.68-7.65]), hypertension (3.07 [1.20-7.84]) and vascular TEAEs (5.27 [1.53-18.18]). Risk factors for vascular TEAEs (HR [95% CI]) were black race compared to white (<0.01 [<0.01-<0.01]), a history of vascular events (4.65 [1.81-11.97]) and cardiac TEAEs (7.73 [2.31-25.84]). In multivariable analyses, treatment group was not predictive of time to initial cardiac (HR 0.87 [95% CI 0.45-1.70]) or vascular (HR 2.17 [95% CI 0.94-45.04) TEAEs. The most common cardiac, vascular, and hypertension TEAEs, respectively, were sinus bradycardia (2.2%), angina pectoris (3.0%) and hypertension (9.7%) with BOS vs electrocardiogram QT prolongation (3.8%), peripheral coldness (1.1%) and hypertension (10.9%) with IMA. One grade 5 cardiac (acute cardiac failure) and one vascular (myocardial ischemia) TEAE were reported with BOS, and one vascular (cerebrovascular accident) TEAE with IMA; none were considered related to study drug.
Successful treatment rechallenge was achieved in the majority of pts with dose interruptions due to cardiac (BOS, 85.7%; IMA, 100%) and vascular (BOS, 100%; IMA, not applicable) TEAEs who were readministered study drug. No pts had dose interruptions due to hypertension TEAEs. Cardiac, vascular and hypertension TEAEs resolved in 57.7%, 75.0% and 35.7% of pts receiving BOS and 65.2%, 66.7% and 48.3% receiving IMA.
Conclusions: In this final analysis of BFORE, the incidence of cardiac, vascular, and hypertension TEAEs in pts with newly diagnosed CP CML receiving BOS or IMA was low and was similar between treatment groups. These AEs infrequently led to treatment discontinuation. In addition to continued improved efficacy with BOS vs IMA after 5 yrs follow-up (Brümmendorf et al., ASH 2020), these safety results support the use of first-line BOS as a standard of care in pts with CP CML.
Cortes:Bristol-Myers Squibb: Research Funding; BiolineRx: Consultancy, Research Funding; Takeda: Consultancy, Research Funding; BioPath Holdings: Consultancy, Membership on an entity's Board of Directors or advisory committees, Research Funding; Pfizer: Consultancy, Research Funding; Amphivena Therapeutics: Research Funding; Arog: Research Funding; Jazz Pharmaceuticals: Consultancy, Research Funding; Telios: Research Funding; Astellas: Research Funding; Sun Pharma: Research Funding; Merus: Research Funding; Daiichi Sankyo: Consultancy, Research Funding; Novartis: Consultancy, Research Funding; Immunogen: Research Funding. le Coutre:Incyte: Honoraria; Pfizer: Honoraria; Novartis: Honoraria. Gambacorti-Passerini:Bristol-Myers Squibb: Consultancy; Pfizer: Honoraria, Research Funding. Hjorth-Hansen:Pfizer: Honoraria, Research Funding; Austrian Orphan Pharma: Honoraria, Research Funding; Bristol-Myers Squibb: Research Funding. Garcia-Gutiérrez:Novartis: Consultancy, Other: Travel, Accommodation, Expenses, Research Funding; Bristol-Myers Squibb: Consultancy, Other: Travel, Accommodation, Expenses, Research Funding; Pfizer: Consultancy, Other: Travel, Accommodation, Expenses, Research Funding; Incyte: Consultancy, Other: Travel, Accommodation, Expenses, Research Funding. Kota:Ariad: Honoraria; Incyte: Honoraria; Xcenda: Honoraria; Novartis: Consultancy, Honoraria; Millennium Pharmaceuticals, Inc., a wholly owned subsidiary of Takeda Pharmaceutical, Company Ltd, Cambridge, MA, USA: Honoraria; Pfizer: Consultancy, Honoraria. Purcell:Pfizer: Current Employment, Current equity holder in publicly-traded company. Viqueira:Pfizer: Current Employment, Current equity holder in publicly-traded company. Leip:Pfizer: Current Employment, Current equity holder in publicly-traded company. Brümmendorf:Takeda: Consultancy; Janssen: Consultancy; Merck: Consultancy; Pfizer: Consultancy, Honoraria, Other: Travel, Accommodation, Expenses, Research Funding; Novartis: Consultancy, Other: travel, accommodation, expenses, Research Funding.
This icon denotes a clinically relevant abstract

